“See one, do one, teach one,” is how a doctor friend explained her medical school training to me. The first time she performed a circumcision on a newborn she was a medical student. She had no idea what she was doing. She took off too much of the baby’s penile tissue. But, she told me, she felt she had no choice. Her mentors expected her to first see the circumcision, then do the circumcision, and then teach other medical students how to perform it.
See one, do one, teach one. You watch a procedure. Then you do that procedure on the next patient. Then you teach other medical students how it’s done.
“Sharp objects, private parts, you have to be really, really careful,” said another doctor friend when we were talking about circumcision and vasectomies, cringing slightly. “You want someone who knows what they’re doing. If not, things are apt to go wrong.”
Circumcision in the United States
In America, circumcision rates vary widely from state to state. The procedure seems to be on the decline. There’s even a name for moms who chose to have it done and now regret it: regret moms. But cutting off the foreskin of a baby boy’s penis is still the norm in many places in the United States.
In Europe circumcision is not the norm. Baby boys’ penises are not operated on within hours or days of birth. In fact, the vast majority of countries in the industrialized world leave babies’ genitals intact.
In America medical students and the nurses who assist them often feel they are witnessing an abusive situation. But they do not feel they can speak up.
A nurse I’ll call Cara works in Upstate New York. She recently told the truth about what newborn boys actually experience when they are circumcised during training days by medical school students doing their pediatric rotation.
To understand Nurse Cara’s account, it’s important to know a little bit about circumcision procedure and techniques. Generally (but not always) for infant circumcision analgesia is given to the baby.
There are three kinds of anesthesia:
- Analgesic cream rubbed onto the baby’s penis
- A penile ring block
- A dorsal nerve block
Some doctors prefer not to use any anesthesia. Some doctors use anesthesia but don’t wait the requisite amount of time for it to numb the area.
As one nurse practitioner confided in me:
I often saw Lidocaine cream applied, but the doctors didn’t wait for it to take effect. They treated circs as something to do if they had a five- or ten-minute window in their schedule. They’d pop into the nursery with little notice, and nurses would quickly put the cream on but then have to wheel the babies down to the circumcision room. You were supposed to wait 20 minutes for it to take effect but they rarely waited. Many doctors didn’t use any anesthetic whatsoever.”
There are different devices used to perform the circumcision. The most commonly used method of circumcision involves the use of a shield and clamp device. The three most commonly used shield and clamp devices are the Gomco circumcision clamp, the Mogen clamp, and the PlastiBell.
The Gomco device has a metal bell that protects the entire head of the penis. It is considered a more difficult device to use because the partially cut foreskin must be threaded between the bell and the clamp frame before the clamp is tightened. Complications arising from the use of this device include bleeding, excessive mucosa, and infection.
The Mogen clamp is the device used in traditional Jewish circumcisions. While it is purportedly associated with fewer complications, one disadvantage is that the device does not directly protect the glans during the procedure. The Mogen clamp design is problematic because the medical school student or doctor is unable to see what they’re cutting. The Mogen clamp has been the subject of numerous lawsuits for laceration, hemorrhaging, and even penile amputations. These are the primary complications. This device is rarely used in hospital settings anymore, due to how easy it is to accidentally amputate the glans on newborn boys.
The Plastibell device is considered easier to use because the plastic ring or bell, once placed on the penis, remains in place until the foreskin becomes necrotic. Then both the ring and the foreskin fall off on their own, which usually takes about 10 days. The primary complication using the Plastibell device is bleeding or infection, usually related to delayed separation of the ring.
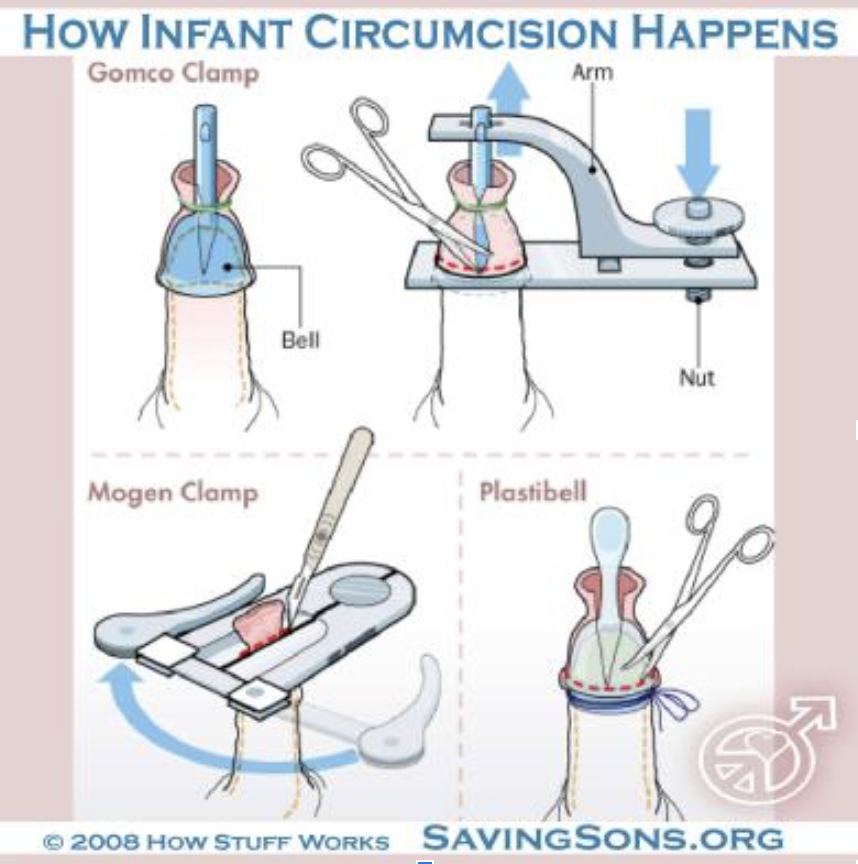
Graphic courtesy of Save Our Sons (via Facebook)
At this point, I should add a trigger warning: Some readers may find the following upsetting and hard to read.
Nurse Cara was scheduled to assist with two circumcisions. Since both were being performed by the same doctor, she set up two boards. These are hard plastic boards with cutouts shaped like babies. They have velcro arm and leg restraints. The infant, who may be naked or may remain clothed but who has his diaper open to expose his penis, is literally strapped down to the hard plastic board.

The practice of circumcision involves strapping a baby down to a hard plastic board. Photo from medical supply company AliMed.com’s webpage.
Then Nurse Cara prepared two sets of equipment in the same room. She wheeled both infants into the room. She strapped the babies down side by side. Their arms and legs bound, their genitals exposed to the air, both newborn boys began to cry.
The doctor entered the room. Two residents, there to learn and observe, trailed behind him. Residents have completed four years of medical school and are now practicing physicians under the supervision of more senior doctors. Residency programs are where doctors learn their speciality. They usually last three years.
The supervising doctor draped a cloth with a hole in it for the penis over the first baby’s genital area and disinfected his privates. He then went over the instruments with the residents and began the procedure. When baby boys are born, the foreskin is snugly attached to the head of the penis. The foreskin detaches naturally as boys grow and develop. In order to perform a circumcision the foreskin must be wrenched away from the penis itself.
The step-by-step process of circumcision
Step one: The doctor inserted a probe between the boy’s foreskin and the glans in order to separate it from the head of the penis. He moved it in a circular motion, explaining each of his actions to the residents. This action is akin to sticking a scalpel under a fingernail and slowly prying it off.
The supervising doctor did this painful step more slowly than usual. He was explaining the process to the residents as he went, all while the baby screamed in pain.
When one newly minted nurse mentioned her concern over the pain newborns feel during circumcision, her attending physician insisted the baby he was circumcising was crying because he was cold. She was also told newborns’ pain receptors aren’t developed yet and that newborns can’t feel pain. This doctor, who did not use any anesthesia, suggested she stick a gloved finger in the baby’s mouth for it to suck on, if the crying bothered her so much. Research from Oxford University shows definitively what every parent knows: infants feel pain, just like adults.
Step two: The doctor then very slowly made a vertical slit with his scissors. In agonizing pain, the newborn baby bucked and pulled at the restraints.
Step three: The doctor then exposed the bleeding red glans further, pointing and making more medical observations. The two trainees looked on intently.
Step four: The doctor then took the bell and placed it over the glans, pulling the skin back over. He placed the rest of the clamp around it, inserted a sterile safety pin and screwed the clamp tight. Under normal circumstances, the doctor would then move on to the next baby and apply a bell and clamp. Instead, he continued to explain the procedure to the residents.
Her anxiety mounting as the doctor and residents ignored the babies’ cries of pain, Nurse Cara tried to nudge the doctor to move more quickly. He ignored her, remaining completely unfazed by the babies’ collective distress.
“The doctors I witnessed do circumcisions seemed to have shut off all feelings,” says Michelle O’Neil, a former postpartum nurse. “The babies were like lab rats to them. Not humans. They would never do to grown men what they were doing to these babies: Operating without any anesthesia in some cases, and without proper anesthesia in others.”
Step five: The doctor then took the scalpel. As the two residents watched closely, he began to make a circular cut. He paused during the procedure to comment, then continued on as the baby wailed.
Step six: The doctor then removed the clamp and bell revealing a completely exposed foreskin-free glans. The doctor made a visual inspection and pointed out some details. He ran his finger around the glans, oblivious to or simply choosing to ignore the even louder cries of the infant. He then told the students to do the same. He continued to make observations about how much exposure of the glans is acceptable. Then he picked up the scissors to remove the frenulum. The frenulum is the small tag of skin on the underside of the penis, like the frenulum you have under your tongue. Like with your tongue, the frenulum anchors the foreskin to the glans.
“One of these two will do the next one, right?” the doctor said lightly, winking at the residents.
Step seven: The doctor then made a snip as the baby bucked in pain. Instead of completing the operation, he again stopped to make observations.
It was obvious to Nurse Cara that this baby was in agony. While this might be a routine medical procedure in America, what she was witnessing was child abuse.
Step eight: Finally, the doctor snipped again, completing the circumcision. The circumcision had taken 25 minutes instead of the usual ten to fifteen. By this time the baby’s cries had turned to whimpers. When the doctor finally finished, the little boy lay limp in the restraints. When a human experiences an extreme trauma like unbearable pain, he will often go into shock. Parents are handed back their newly circumcised baby and told that he is “sleeping.” which is not what is actually happening. When a circumcision is done like this, the baby often becomes catatonic from shock. Nurse Cara then put gauze slathered with petroleum jelly over the first baby’s bleeding penis, wishing she could find some way to comfort him.
Most parents are not in the room when their infant is circumcised. They do not realize how traumatizing and painful the operation can be. The nurse returns the baby back to them “asleep.” So parents say to themselves: “It must not have been too bad. He seems fine. He seems perfectly content.”
See one, do one
As Nurse Cara continued to watch, the supervising doctor turned to the next baby and asked the two residents “Which one of you wants to try?”
One of the residents stepped forward. Remember the second infant had been strapped down for 25 minutes listening to the cries of the first. He had been crying and whimpering that entire time, before his operation even started.
The resident sterilized the second baby’s genital area. He separated the foreskin from the glans with a metal probe, paused, and looked up for reassurance from his supervisor, who nodded.
The baby’s screams intensified. Again the doctor and the students appeared not to notice. The resident made a dorsal cut and placed the bell over the glans.
He attached the clamp as the doctor coached, “Good, now draw the foreskin up, a little further…. great! Now secure it with the pin…” The trainee fumbled, inserting the pin through only part of the foreskin.
The doctor stopped him: “No, through both sides, take it out and try it again.”
Nurse Cara felt her heart in her throat. This baby had already been stabbed once, only to have to suffer through more pain due to the resident’s incompetence and inexperience. When parents sign those consent forms in a teaching hospital they are unknowingly consenting to medical students practicing surgery on their newborns. They don’t realize that, like with this resident, their precious new baby may be a guinea pig for a medical student or inexperienced physician.
On his second try, the trainee completed the insertion. He secured the clamp, tightening the bolt as the baby screamed. He let go as the clamp did its work. “That wasn’t too difficult,” the doctor commented. “Now all you have to do is….” and he went on to describe the rest of the procedure.
After this lengthy explanation, the second baby’s foreskin was excised.
But when the clamp was removed this time Nurse Cara noticed that there was hardly any skin or slack left on the baby. Instead of a normal-looking penis, this baby had an exposed glans on a shaft which stuck straight up with tension.
The supervising doctor examined the work with a frown. “It’s a little tight” he said, “next time try not to take off quite so much.”
The resident then proceeded to snip the frenulum. As he made the cut, the baby again screamed in pain.
Instead of taking off too much, this time the resident took off too little. The doctor observed and noted that he had “missed a bit.” He instructed him to make another cut. The resident complied and the rest of the frenulum was removed from the screaming infant.
“Well that’s it for the procedure. You all understand it?” The doctor said.
Both residents both nodded eagerly.
“Well then I’ll see you both tomorrow, and you’ll get a try,” he said pointing to the second resident.
Without a backwards glance at the two infants, the doctor and the two residents walked away. They had inflicted tremendous pain on both. One had a mutilated penis that would likely cause him painful erections for the rest of his life. These boys’ parents had no idea what their sons had just gone through. But for the supervising doctor and the two residents this was all in a day’s work.
How can it be okay to hurt baby boys in this way?
How would those babies’ parents feel if they knew that totally inexperienced residents were operating on their babies’ genitalia? Michelle O’Neil once saw a nervous med student take 45 minutes to perform a circumcision.
When the United Kingdom nationalized their health care system after World War II, routine circumcision of newborn babies ended virtually overnight.
If you do a deep dive into the research, you learn that the most scientific, most ethical, and kindest decision is not to circumcise your baby boy. Yet here we are in 2020 in America continuing a painful and unnecessary practice in the name of “medicine.”
Related posts:
12 Reasons Why the AAP is Right and You Should Circumcise Your Son
1 in 500 Boys Will Experience Acute Complications
Circumcision Pros and Cons: One Mom’s Regret
This breaks my soul. I’m traumatised. Those poor babies. Who will avenge them?
This story is absolutely heartbreaking. I am so glad that I decided (against my ex-husband and his families wishes) not to circumcise both of my sons. Ironically, they called me a barbarian for not doing so. The level of trauma, pain and suffering inflicted on these precious souls from the very day they come into this world by the draconian medical system is shocking. How ignorant doctors can just disconnect from the pain and suffering that they’re inflicting on these babies and say that they can’t feel anything?!!! Obviously, to make themselves and their conscience feel better. I really want people to wake up and question everything. Especially standard of care medicine, which is the 3rd leading cause of death.